Quick Facts
- Primary Symptom: Sharp, stabbing chest pain is the most frequent symptom, occurring in 85% to 90% of all cases.
- Positional Relief: Pain typically improves when sitting up and leaning forward, and worsens when lying flat.
- Clinical Significance: Acute pericarditis is responsible for approximately 5% of all emergency department admissions for chest pain in North America and Western Europe.
- Common Triggers: Often follows a recent viral or respiratory infection, a condition known as a viral prodrome.
- Risk of Recurrence: Between 15% and 30% of individuals diagnosed with acute pericarditis experience at least one recurrent episode within 18 months of the initial event.
- Treatment Standard: Management focuses on reducing inflammation using medications like NSAIDs and colchicine.
- Medical Urgency: Any new or severe chest pain requires immediate evaluation to rule out life-threatening conditions.
Pericarditis symptoms typically include sharp, stabbing chest pain caused by inflammation of the heart's protective lining, the pericardium. This pain uniquely intensifies when breathing deeply or lying flat and may improve when sitting up and leaning forward, making it crucial to understand how to tell if chest pain is pericarditis or something more life-threatening like a heart attack.
The Signature Pain: Recognizing Pericarditis Signs
When we talk about men’s health and longevity, the heart is always at the center of the conversation. One condition that often mimics the terror of a heart attack but has a very different clinical profile is pericarditis. This is an inflammation of the heart sac, the thin, two-layered membrane that surrounds your heart. In a healthy state, these layers glide over each other with a small amount of fluid between them. When they become inflamed, they rub together like two pieces of dry leather, creating a specific type of discomfort known as pleuritic pain.
For most men, the first sign is a sudden onset of sharp chest pain when breathing or lying flat. Unlike the dull pressure often associated with cardiac artery issues, this sensation is often described as knife-like. It is typically felt behind the breastbone or on the left side of the chest. A hallmark of the condition is how it reacts to your posture. If you find that leaning forward provides a measure of relief, while lying flat on your back makes the pain unbearable, you are likely dealing with the classic positional relief associated with an inflamed pericardium.
In many instances, these issues do not appear in a vacuum. You might notice pericarditis symptoms after viral infection, such as a recent bout with the flu or a lingering respiratory bug. During this period, you may also experience a viral prodrome including a low-grade fever, general weakness, and a dry cough. The pain can also radiate, much like a heart attack, moving into the left shoulder or the trapezius ridge. This occurs because the phrenic nerve, which supplies the pericardium, also travels to these areas of the upper body.
Is It Pericarditis or a Heart Attack?
For any man over 40, chest pain is a "red flag" that demands immediate attention. However, understanding the difference between pericarditis vs heart attack symptoms can help you provide clearer information to emergency responders. While both are serious, a heart attack is an immediate plumbing issue—a blocked artery—whereas pericarditis is an inflammatory issue.
The table below outlines the primary clinical differences:
| Feature | Pericarditis | Heart Attack (Myocardial Infarction) |
|---|---|---|
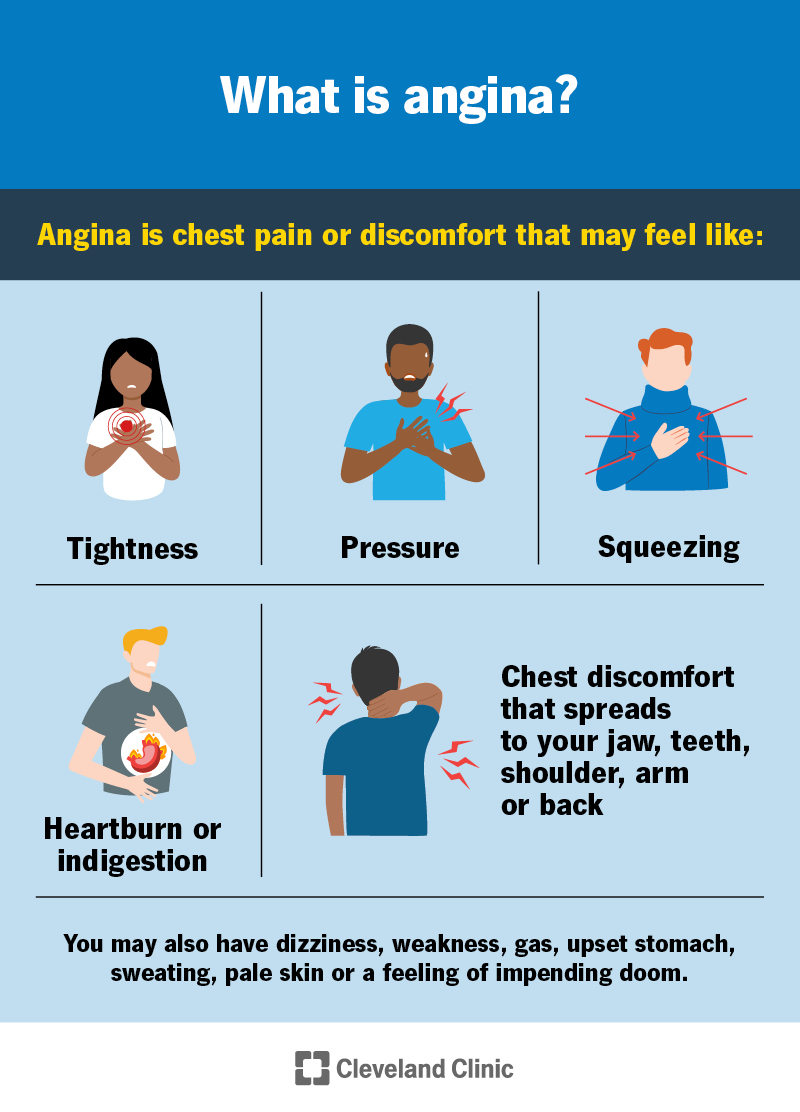
| Pain Quality | Sharp, stabbing, or piercing | Heavy pressure, squeezing, or "elephant on chest" |
| Positional Change | Improves leaning forward; worsens lying flat | No change with position |
| Breathing Impact | Pain increases with deep breaths (pleuritic) | Generally no change with deep breaths |
| Onset | Often follows a viral illness; can be gradual | Often sudden; can occur during physical exertion |
| Radiation | Left shoulder, neck, trapezius ridge | Left arm, jaw, neck, or back |
| Duration | Can last for days or weeks constant | Usually episodic or intensifying over minutes/hours |
It is important to note that you cannot diagnose yourself. Even if your symptoms align perfectly with the pericarditis column, medical professionals treat all chest pain as a heart attack until proven otherwise. In some cases, a specific form of pericarditis called Dressler syndrome can actually occur weeks after a heart attack or heart surgery, representing the body's delayed immune response.
Red Flag Call-Out: Seek emergency care immediately if you experience crushing chest pressure, sudden shortness of breath, profound sweating, or pain that radiates to the jaw. Do not wait to see if the pain changes with position if it is severe.
The Medical Path: Diagnosis and Testing
If you present at the emergency department with these symptoms, the clinical team will initiate a pericarditis medical diagnosis protocol. This usually begins with a physical exam. Using a stethoscope, a doctor listens for a pericardial friction rub—a high-pitched, scratchy sound produced by the inflamed layers of the heart sac rubbing against each other. This sound is best heard when the patient is leaning forward and holding their breath.
The diagnostic journey typically involves several key tests:
- Electrocardiogram (ECG): This tracks the electrical activity of your heart. Pericarditis often shows specific ST-segment elevations that are widespread across several leads, which helps doctors distinguish it from the localized changes seen in a heart attack.
- Blood Tests: Doctors look for elevated inflammatory markers in your blood, specifically C-reactive protein (CRP) and the erythrocyte sedimentation rate (ESR). They may also check troponin levels to ensure there is no damage to the heart muscle itself.
- Echocardiography: This ultrasound of the heart is used to check for fluid buildup between the layers of the pericardium, a condition known as pericardial effusion.
- Advanced Imaging: In complex cases, a Cardiac MRI or CT scan may be used to look for thickening or calcification of the heart sac.
Accurate diagnosis is vital for long-term longevity. Chronic inflammation that goes untreated can lead to more serious complications, so the goal of the medical diagnosis is not just to stop the pain, but to identify the underlying cause and prevent future episodes.
Treatment and Preventing Recurrence
Once the diagnosis is confirmed, management typically focuses on aggressively curbing the inflammation. The standard pericarditis treatment with nsaids and colchicine is the first line of defense. High-dose aspirin or ibuprofen is used to reduce the immediate pain and swelling, while colchicine—a drug traditionally used for gout—has been shown to significantly reduce the risk of the condition returning.
Recurrence is a major concern for patients. Statistics show that between 15% and 30% of individuals diagnosed with acute pericarditis experience at least one recurrent episode within 18 months of the initial event. To minimize this risk, doctors often emphasize the importance of physical activity restriction. For a man used to a high-intensity workout routine, this can be the hardest part of the recovery. However, pushing your heart rate too high while the pericardium is still inflamed can trigger a relapse or lead to chronic issues.
In more persistent or recurrent pericarditis symptoms and management cases, newer therapies are coming to the forefront. By 2025 and 2026, we are seeing increased use of Anti-IL1 agents, which target specific pathways in the immune system to stop the cycle of inflammation. Corticosteroids like prednisone are generally reserved for those who do not respond to first-line treatments, as they can sometimes increase the risk of future recurrences if tapered too quickly.
Finally, patients must be aware of cardiac tamponade symptoms to watch for. This is a rare but life-threatening complication where too much fluid builds up in the heart sac, preventing the heart from filling properly. If you experience sudden, extreme shortness of breath, dizziness, or a feeling that you might faint, it requires immediate surgical intervention to drain the fluid.
FAQ
How can you tell the difference between pericarditis and a heart attack?
The most reliable way to tell the difference is the nature of the pain and its response to movement. Pericarditis pain is usually sharp and stabbing and changes when you shift positions or breathe deeply. Heart attack pain is more often described as a heavy pressure or squeezing sensation that does not change when you sit up or lean forward. Because these symptoms can overlap, any severe chest pain must be evaluated by a medical professional immediately.
Does pericarditis pain get worse when lying down?
Yes, intensified pain when lying flat is a classic symptom of pericarditis. This happens because the position causes the inflamed layers of the pericardium to press more firmly against each other or changes the way the heart sits in the chest cavity. Sitting upright or leaning forward typically pulls the heart away from the front of the chest, which often provides significant relief from the sharp sensation.
Where is pericarditis pain usually felt?
Pericarditis pain is most commonly felt behind the breastbone or on the left side of the chest. However, because of the way nerves are distributed in the chest and neck, the pain can radiate to the left shoulder and the trapezius muscles. This radiation to the shoulder ridge is a very specific sign that doctors look for during a clinical evaluation.
What does pericarditis chest pain feel like?
Most patients describe the pain as a sharp, piercing, or stabbing sensation. It is often called pleuritic pain because it feels worse when you take a deep breath, cough, or swallow. While it can occasionally feel like a dull ache, the sharp, knife-like quality is the most frequent presentation, especially during the acute phase of the inflammation.
When should you see a doctor for pericarditis symptoms?
You should seek medical attention the moment you experience any new, unexplained, or severe chest pain. While pericarditis itself is often manageable with medication, it requires a professional diagnosis to rule out a heart attack or pulmonary embolism. Furthermore, you should see a doctor immediately if you have been diagnosed with pericarditis and develop new symptoms like extreme shortness of breath, swelling in the legs, or fainting, as these could indicate a serious complication.
Pursuing Long-Term Vitality
Maintaining your heart health isn't just about surviving an acute episode; it’s about proactive prevention. If you’ve experienced pericarditis, focus on a heart-healthy diet rich in anti-inflammatory foods, manage your stress levels, and strictly follow your doctor’s guidance on returning to exercise. By understanding the signals your body sends and responding with research-backed strategies, you can protect your vitality and ensure your heart stays strong for the long haul.