Quick Facts
- Prevalence: A study assessing middle-aged females found that approximately 45% of the subjects exhibited some degree of lumbar hyperlordosis.
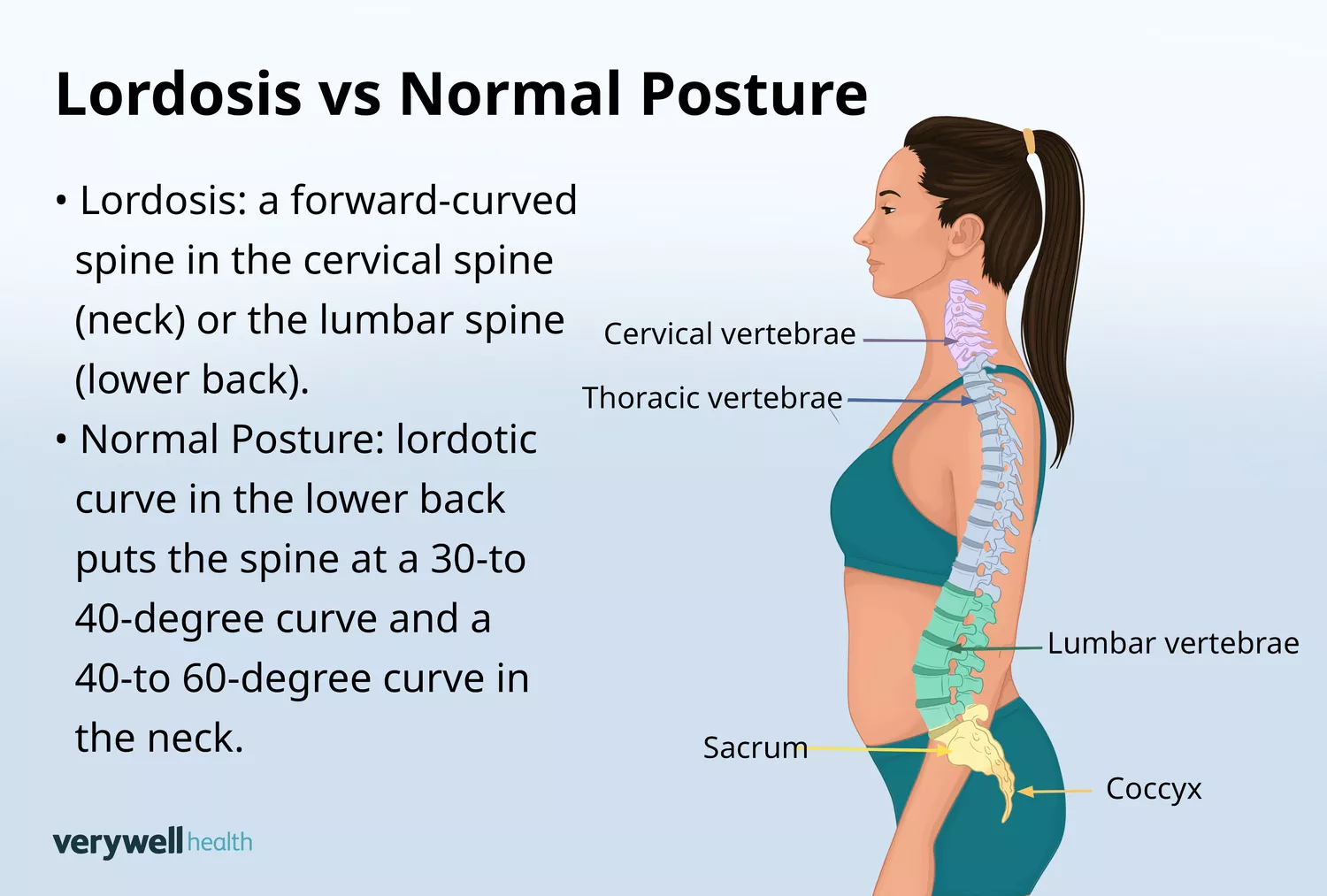
- Normal Range: The Scoliosis Research Society defines the normal range for lumbar lordotic curvature as being between 40 and 60 degrees.
- Pelvic Tilt Benchmark: A forward pelvic rotation exceeding 8 or 9 degrees is clinically recognized as excessive anterior pelvic tilt.
- Recovery Window: Most athletes and patients see significant postural improvement within 8 weeks of consistent corrective training.
- Core Strategy: Successful management requires a "push-pull" approach—stretching overactive hip flexors while aggressively strengthening the glutes and deep core.
- Daily Awareness: Simple modifications in how you sit and sleep can prevent the progression of habitual postural lordosis.
Lordosis posture correction focuses on restoring neutral spine alignment by strengthening weak core and gluteal muscles while stretching tight hip flexors. To address hyperlordosis, individuals should practice abdominal bracing and posterior pelvic tilts to counteract excessive lower back curvature. Consistent awareness of pelvic rotation during daily activities is essential for maintaining musculoskeletal balance and reducing lower back pain.
Diagnostic Check: Do You Have Hyperlordosis?
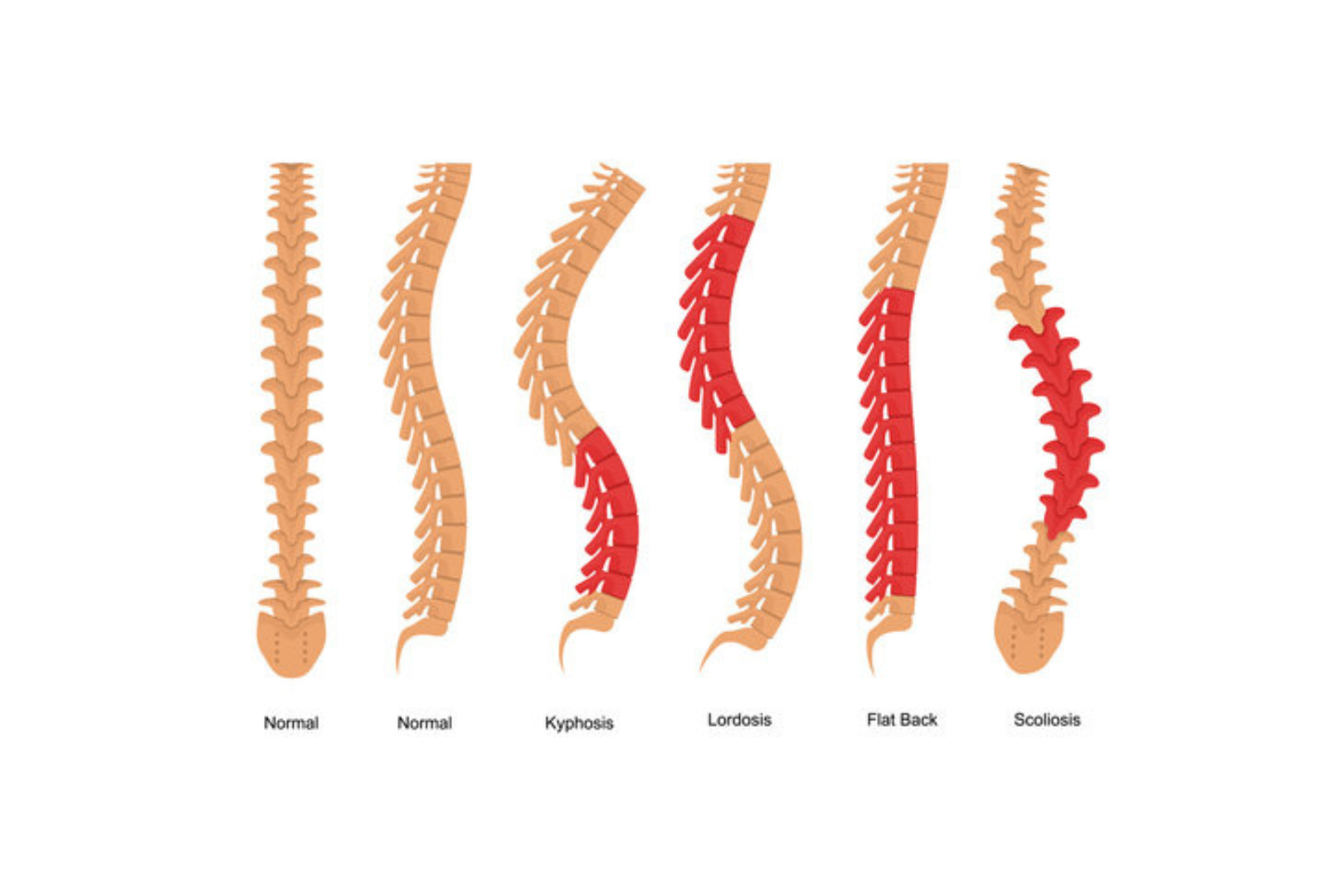
Before diving into a training program, you need to understand the current state of your lumbar spine. Hyperlordosis, often called "swayback" or "hollow back," occurs when the inward curve of your lower back becomes exaggerated. This often forces the abdomen forward and the buttocks backward, creating a noticeable C-shape in the profile.
A simple way to start is the Floor Test. Lie flat on your back on a hard surface. If you can slide your entire hand easily between the floor and your lower back with room to spare, you likely have an increased lumbar curve. For a more clinical assessment, professionals use the Thomas Test. Sit at the very edge of a sturdy table, hug one knee to your chest, and slowly lie back. If your extended leg lifts off the table, it indicates significant hip flexor tightness, a primary driver of pelvic rotation.
It is important to distinguish between postural lordosis and structural lordosis. Postural issues are habitual, usually caused by a sedentary lifestyle or poor training form, and are highly responsive to lordosis posture correction routines. Structural issues are often congenital or related to bone density, requiring more specialized medical intervention. Regardless of the cause, identifying the degree of anterior tilt is the first step toward lower back pain relief for lordosis patients.
Pro Tip: The Thomas Test When performing the Thomas Test, have a partner observe the angle of your hanging leg. If the thigh remains above the horizontal plane of the table, your psoas and iliacus are likely shortened, pulling your pelvis into a permanent forward tilt.
The Correction Matrix: Stretches for Excessive Spinal Curvature
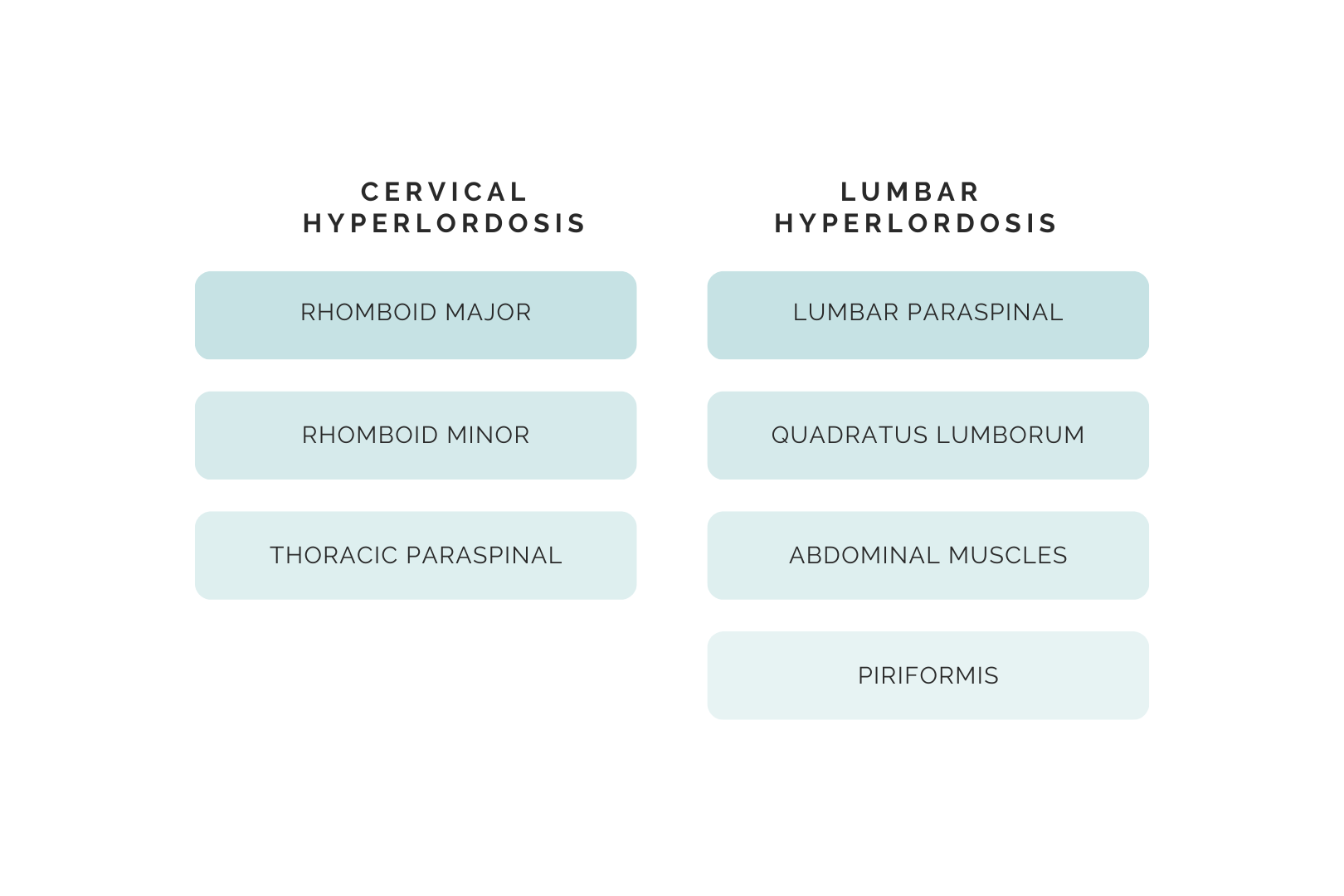
To fix a curve that has gone too far, we must first address the "tether" pulling the pelvis forward. In most modern athletes and office workers, the hip flexors (the psoas and iliopsoas) and the quadriceps are chronically short and tight. This creates a phenomenon known as Gluteal Amnesia, where the brain "forgets" how to effectively fire the glute muscles because the opposing muscles are so tight.
Incorporate these daily stretches for excessive spinal curvature to release the front of the hips:
- Kneeling Hip Flexor Stretch: Drop into a lunge with one knee on the ground. Tuck your tailbone under (posterior pelvic tilt) and gently shift your weight forward. You should feel a deep stretch in the front of the hip. Hold for 30 seconds per side and repeat for 3 sets.
- Half-Kneeling Quad Release: Similar to the hip flexor stretch, but elevate your back foot onto a bench or couch. This adds intensity by targeting the rectus femoris. Focus on abdominal bracing to keep your back from arching during the stretch.
- The 90/90 Stretch: Sit on the floor with one leg bent at 90 degrees in front of you and the other at 90 degrees to the side. Lean slightly forward to open up the hip capsule.
Stretching alone is not a cure, but it "unblocks" the pelvis, allowing for better musculoskeletal balance. When you release these tight tissues, you create the mechanical space necessary for the glutes and abdominals to actually do their job during pelvic tilt exercises for lordosis.
Strengthening the Foundation: Pelvic Tilt Exercises for Lordosis
Once the front is loose, we must strengthen the back and the core. The goal is to build enough tension in the gluteus maximus, hamstrings, and rectus abdominis to pull the pelvis back into a neutral position. This is the core of lordosis posture correction.
The following routine focuses on sensorimotor control—teaching your brain to find and hold a neutral spine alignment.
1. Posterior Pelvic Tilts
This is the fundamental movement for lordosis posture correction. Lie on your back with knees bent. Flatten your lower back against the floor by contracting your abs and tilting your hips upward.
- Dosage: Hold for 10 seconds, perform 15 repetitions.
2. The Dead Bug
This is the gold standard for core strengthening exercises for anterior pelvic tilt. Lie on your back with arms and legs in the air, knees bent at 90 degrees. Slowly lower the opposite arm and leg toward the floor while keeping your lower back pressed firmly against the ground. If your back arches, you’ve gone too far.
- Dosage: 3 sets of 10 slow reps per side.
3. Glute Bridges
Activating the posterior chain is vital for strengthening weak glutes for posture correction. Lie on your back, feet flat on the floor. Lift your hips until your body forms a straight line from knees to shoulders. Squeeze your glutes hard at the top without over-arching your lower back.
- Dosage: 3 sets of 15 reps, focusing on a 2-second hold at the top.
4. Hardstyle Plank
A standard plank is good, but a "hardstyle" plank is better for spinal stability. Get into a forearm plank position. Squeeze your glutes as hard as possible and pull your elbows toward your toes (without actually moving them). This creates maximum tension in the obliques and transverse abdominis.
- Dosage: 3 sets of 30 seconds.
Lordosis Management: Lifestyle Tips for Daily Life
Training for 30 minutes a day cannot always overcome 23 hours of poor habits. Effective lordosis management lifestyle tips focus on changing how you interact with your environment. If you work a desk job, you are at a higher risk for hip flexor tightness due to a sedentary lifestyle.
For office workers, implementing lumbar lordosis ergonomic desk setup tips is a game-changer. Ensure your chair provides adequate lumbar support, but more importantly, adjust your seat height so your hips are slightly higher than your knees. This reduces the constant "shortening" of the hip flexors. Utilize a standing desk for part of the day, but be wary of "leaning" into your lower back, which can worsen the curve.

Sleep is another area where minor tweaks offer major benefits. Finding the best sleeping positions for lumbar lordosis relief is about maintaining a neutral spine while you're unconscious. If you sleep on your back, place a medium-sized pillow under your knees. This slightly flexes the hips and flattens the lumbar spine against the mattress. For side sleepers, draw your knees up slightly and place a pillow between them to keep the hips and pelvis level, preventing pelvic rotation.

Pro Tip: The 8-Degree Rule In a professional setting, a pelvic tilt is measured using the angle between the Anterior Superior Iliac Spine (ASIS) and the Posterior Superior Iliac Spine (PSIS). If the front of your hip bone is significantly lower than the back (more than 8-9 degrees), your priority should be posterior tilt strengthening.
When to See a Professional: The Treatment Ladder
If consistent lordosis posture correction exercises do not alleviate your pain or improve your silhouette after 10-12 weeks, it is time to climb the treatment ladder. Chronic hyperlordosis can lead to degenerative changes in the lumbar spine or disc herniations if left unchecked.
A doctor or specialist may recommend diagnostic imaging, such as a side-view X-ray, to measure the exact degree of your curve. If there is radiating pain or numbness in the legs, an MRI may be necessary to check for nerve compression. Physical therapy is often the next step, providing manual therapy to release deep tissue and guided neuromuscular re-education. In rare, severe cases where structural deformity causes neurological deficit, surgical options like spinal fusion might be considered, though this is a last resort.

FAQ
Can lordosis posture be corrected?
Yes, in most cases, lordosis is postural and can be significantly improved or fully corrected through targeted exercise and lifestyle changes. By balancing the tension between the front and back of the pelvis, you can restore a neutral spine.
What exercises help fix lordosis?
The most effective movements are those that promote a posterior pelvic tilt. These include the dead bug, glute bridges, planks, and bird-dogs. These exercises engage the core and glutes to pull the pelvis out of an excessive forward tilt.
How long does it take to see results from lordosis correction?
With a consistent daily routine, most individuals begin to feel less lower back strain within 2 to 4 weeks. Visible changes in posture and spinal alignment typically take about 8 to 12 weeks of dedicated strengthening and stretching.
Is lordosis the same as anterior pelvic tilt?
They are closely related but not identical. Anterior pelvic tilt refers specifically to the rotation of the pelvis, while lordosis (specifically hyperlordosis) refers to the resulting inward curve of the lumbar spine. An anterior pelvic tilt is almost always the primary cause of postural hyperlordosis.
What is the best sleeping position for lordosis?
The most supportive position is sleeping on your back with a pillow placed under your knees. This position reduces the pull on the hip flexors and allows the lower back to relax into a more neutral alignment.
Can tight hip flexors cause lordosis?
Yes, tight hip flexors are one of the leading causes of postural lordosis. Because the hip flexors attach to the lumbar spine and the pelvis, when they become short and tight, they physically pull the pelvis forward and the spine into a deeper arch.